By Teresa Johnson, MSPH, RD
A symposium chaired by Bahram Arjmandi, PhD, RD, and Carmen Castaneda-Sceppa, MD, PhD, provided insights into the etiology and pathophysiology of osteosarcopenic obesity, and presented suggestions for pharmacological and dietary treatment strategies.
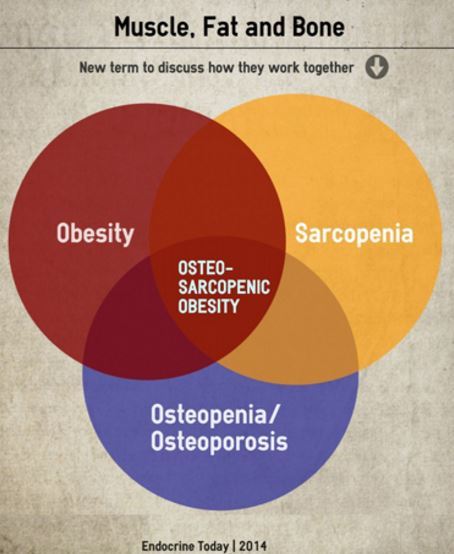
Jasminka Ilich-Ernst, PhD, RD, a professor at Florida State University, outlined the problem and scope of osteosarcopenic obesity, a term first coined in 2012. Characterized by the coexistence of three distinct musculoskeletal disorders—osteopenia/osteoporosis, sarcopenia, and obesity—osteosarcopenic obesity is a complex condition, for which the proof-of-concept was established only recently.
A major concern with osteosarcopenic obesity, Ilich-Ernst said, lies in age-related fat redistribution and subsequent infiltration into bone and muscle. Typically bone, muscle, and fat progenitor cells differentiate in a balanced distribution to enable normal tissue development. But with aging, a sedentary lifestyle, poor nutrition, and low-grade inflammation, differentiation patterns become altered and fat production predominates.
Whereas current nutritional and lifestyle management recommendations address the individual components of osteosarcopenic obesity, they do not address the collective triad. Ilich-Ernst suggested adhering to current recommendations to achieve peak bone mass before age 30, gain and maintain adequate muscle mass, and maintain a health weight, but she added that increasing dietary protein to 25 percent of total energy and limiting carbohydrate consumption to approximately 40 percent of total energy might further reduce risk of developing osteosarcopenic obesity.
Further insights into the interconnected nature of bone, muscle, and fat were provided by Clifford J. Rosen, MD, a professor of medicine at Tufts University and research scientist at the Maine Medical Center Research Institute. Rosen explained that the three tissues derive from a single progenitor cell type, and their responses to various cytokines, hormones, and regulatory input, primarily the sympathetic nervous system, are similar.
He then described newly identified “beige,” or brown-like, adipocytes, which contain more mitochondria and are more thermogenic than classic white adipocytes. Beige adipocytes share a common progenitor cell with smooth muscle. As such, they can be viewed as a sort of “hybrid” between fat and muscle cells. Intermittent cold exposure induces beige adipogenesis, a process referred to as “browning,” and promotes weight loss by increasing sympathetic tone—a potential non-pharmacological approach to body fat loss.
However, Rosen noted, whereas sympathetic tone enhances fat loss, it uncouples the process of bone remodeling, promoting bone loss. He added that many of the new classes of drugs that target beige adipogenesis might have similar, deleterious off-target effects on bone.
Ronenn Roubenoff, MD, MHS, of Novartis Institutes for Bone Research, and a professor of medicine and nutrition at Tufts University, compared the effects of dietary versus pharmacological approaches to treating sarcopenia. Sarcopenia, Roubenoff said, is an age-related loss of muscle mass due to type II muscle fiber atrophy. He said that preventing sarcopenia might increase life span and improve quality of life in older adults.
Although some research suggests increasing dietary protein intake might reduce muscle wasting, few data support changing current recommendations, Roubenoff said. In addition, the muscle-sparing effects of dietary protein differ in women versus men. Whereas women benefit from increased intake, men (who experience a U-shaped curve in response to intake) benefit from more moderate intake.
Roubenoff added that muscle, unlike other organs, doesn’t senesce; rather, it remains plastic, providing the potential for older adults to regain muscle mass and function. However, muscle in older adults exhibits “anabolic resistance”—an inability to integrate and build muscle. Emerging pharmacological approaches target this resistance to reverse muscle wasting.
Finally, Wayne Campbell, PhD, a professor of nutrition science at Purdue University, described the differential effects of dietary protein intake during weight loss on bone, muscle, and fat. Specifically, Campbell addressed the question of how older adults can purposefully lose weight without compromising musculoskeletal function.
Campbell and his colleagues analyzed NHANES data from 1999-2004, a period that included dual energy X-ray absorptiometry data. They partitioned the data based on thresholds of the Recommended Dietary Allowance regarding bone health, and noted that whereas inadequate protein intake had an adverse effect on bone health in adults over age 50, high protein had variable effects. Campbell then described his research with whey supplementation and noted that groups that consumed higher amounts of a whey protein supplement lost more fat than groups consuming lesser amounts. However, they experienced no change in bone status, consistent with the epidemiological data.
At a minimum, Campbell said, adults should consume adequate protein. But he added that high dietary protein intake during weight loss has a positive effect on body composition, inducing greater fat loss while maintaining lean muscle mass. In addition, he noted that high protein intake has variable effects, depending on protein type. In particular, whereas protein from dairy and plant sources likely provides greater benefit to bone, protein from non-dairy animal sources likely benefits soft tissue.